


New government findings add details to the lack of availability of behavioral health services for America’s poor and elderly.
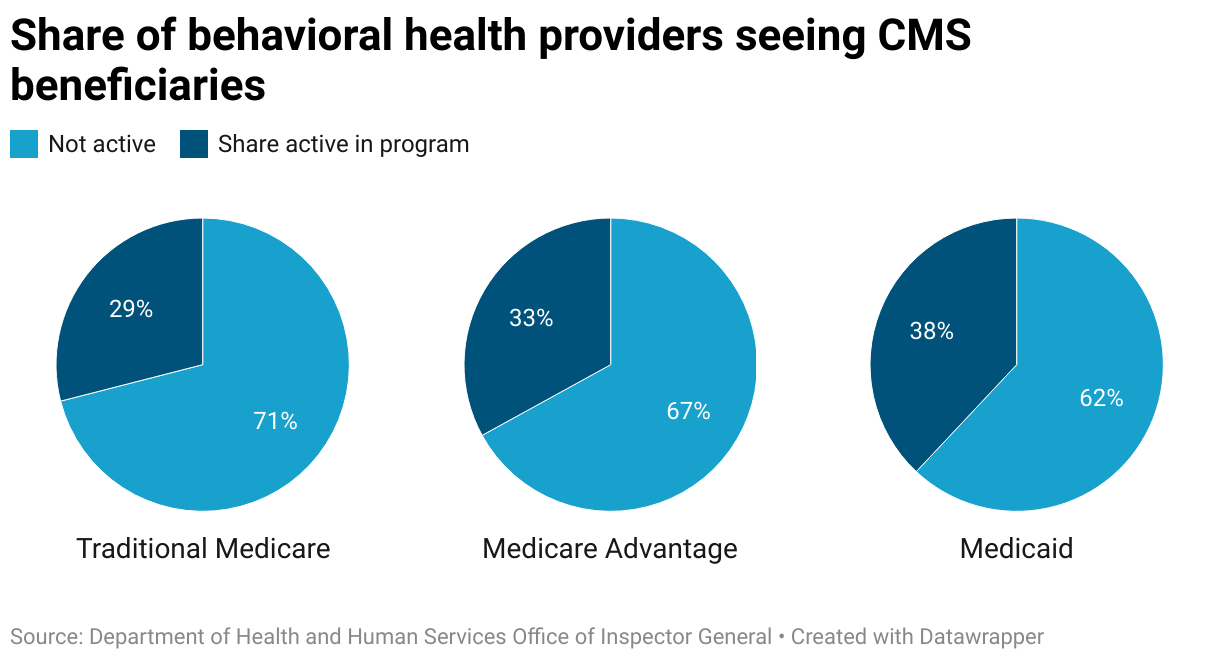
The Office of Inspector General (OIG) for the U.S. Health and Human Services Department found that about one-third of behavioral health providers in selected counties serve patients in the Medicare, Medicare Advantage, or Medicaid programs.
“Despite unprecedented demand for behavioral health services, treatment rates in all three programs remained relatively low,” the OIG said in a new report. “A large barrier to accessing behavioral health care is that there are not enough behavioral health providers in many parts of the country to meet the need for behavioral health services.”
The report studied 20 counties — 10 rural and 10 urban — across 10 states. Specifically, it examined the ratio of providers actively seeing program enrollees to the number of enrollees in Medicare, Medicare Advantage or Medicaid, as well as rates of care use, and telehealth versus in-person services. The time frame was the year 2021.
The report focuses on a time before significant action by the agency that oversees the three programs, the Centers for Medicare & Medicaid Services (CMS), and the White House and Congress. CMS’s response is attached to the report. The agency concurs “with the intent” of OIG’s recommendations.
Utilization and provider trends
The lack of providers serving beneficiaries in the three programs translates to lower use of the behavioral health system. Only 8% of Medicaid enrollees and less than 4% of Medicare and Medicare Advantage enrollees received behavioral health services. The lack of utilization likely belies the need for the services, the report states.
“In the United States, about one in five adults has a mental illness but less than half of those receive services,” the report states.
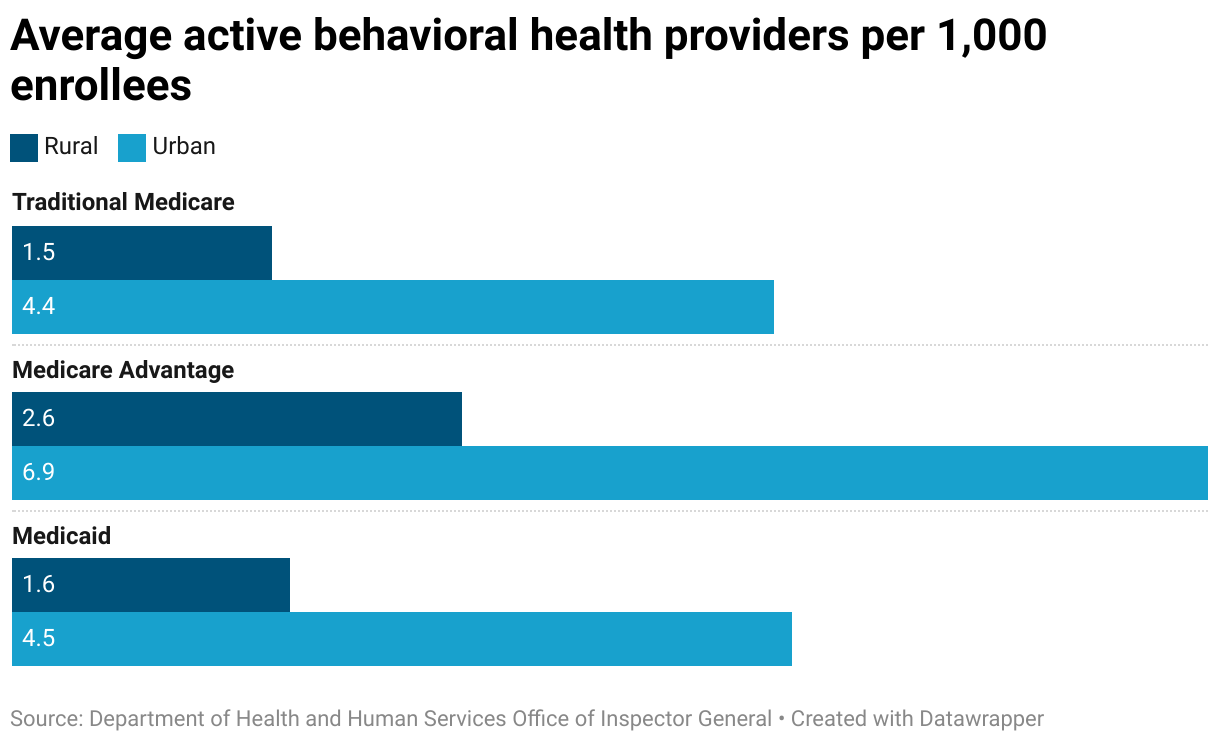
The lack of access to providers is most acute for rural communities. On average, there are fewer than five providers per 1,000 enrollees across the three programs and counties, regardless of type. Traditional Medicare and Medicaid saw the lowest ratios of providers that are active in them.
On average, most enrollees across the programs only saw one provider, rather than different providers, over the course of the year. Medicare members, on average, saw their behavioral health provider eight times a year. For Medicare Advantage, it was five times a year, and Medicaid, six times.
These counties see an even smaller share of providers that can prescribe medication.
“On average, in the selected counties, there were fewer than two active providers who could prescribe medication per 1,000 enrollees in each program,” the report states. “In addition, there were three counties with no active providers who could prescribe in Medicaid, two counties with no active providers who could prescribe in traditional Medicare, and one county with no active providers who could prescribe in Medicare Advantage.
“Similarly, there were 61 Medicare Advantage plans and 20 Medicaid managed care plans offered in the selected counties that had no active prescribers in that county.”
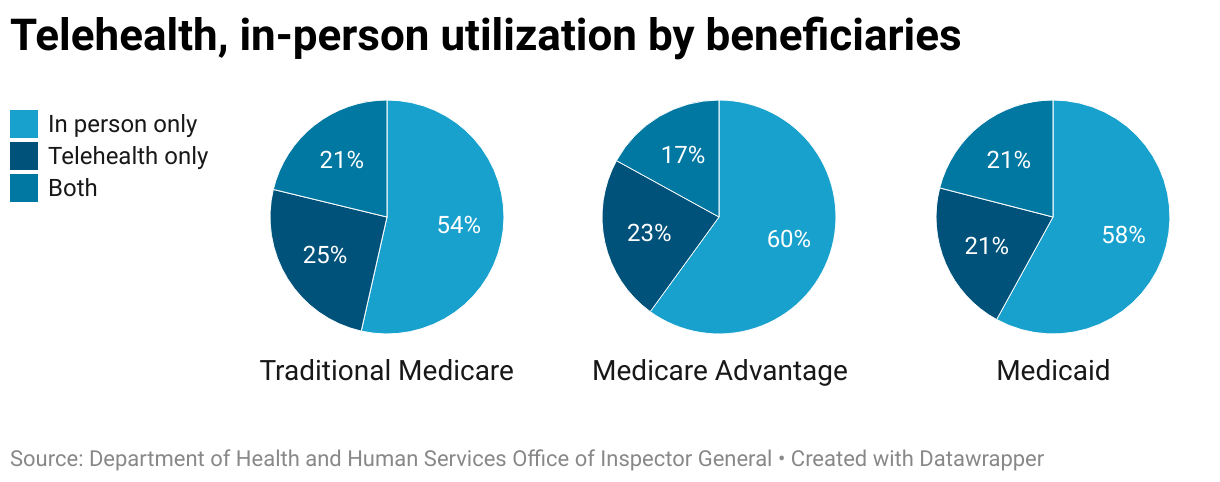
Telehealth utilization varies most between rural and urban counties, with the latter seeing much greater utilization. Across all members, about three-quarters of beneficiaries saw a provider in person at least once in the year, including those who also saw their providers via telehealth, and between a half and two-thirds saw their providers exclusively through telehealth.
Causes and recommendations
Medicare spends an estimated $27 billion a year on behavioral health services, while about 1-in-4 members are coping with a behavioral health condition. For Medicaid, the cumulative spending totals about $52 billion, while adult members experience mental health conditions at a rate of 29% and substance use disorders (SUD) at about 21%, the report states.
Some of the causes of the shortage are well-known in the industry: the administrative burden of participating in certain health plans (especially the prior authorization and credentialing processes), low payment rates by payers and overall provider shortages.
“To move toward parity between behavioral health and physical health services and advance whole-person care in the [Medicare Advantage] program, CMS has finalized policies to require that care coordination programs established by MA organizations (MAOs) include behavioral health services,” CMS’ response states. “CMS also finalized policies for 2024 to strengthen network adequacy requirements, such as adding licensed clinical social workers and clinical psychologists as specialty types for which CMS sets Medicare Advantage plan network adequacy standards, reaffirming MAOs’ responsibilities for behavioral health services and codifying wait-time standards, among other policies.”
OIG recommends four things:
— Take steps to encourage more behavioral health providers to serve Medicare and Medicaid enrollees
— Explore options to expand Medicare and Medicaid coverage to additional behavioral health providers
— Use network adequacy standards to drive an increase in behavioral health providers in Medicare Advantage and Medicaid
— Increase monitoring of Medicare and Medicaid enrollees’ use of behavioral health services and identify vulnerabilities
“To encourage additional behavioral health providers to actively serve enrollees, CMS should also take steps to more accurately value and pay for behavioral health services,” the report states. “When possible, CMS or states should attempt to address significant disparities in payment rates in order to increase the number of providers actively serving enrollees.”
More providers can now be reimbursed for services provided to Medicare beneficiaries. Last year, CMS established rules allowing licensed marriage and family therapists (LMFTs) and mental health counselors into the program, expanding the potential workforce for Medicare recipients.
The several changes that CMS and Congress have made have attracted attention from some telehealth companies. In the last few months, Talkspace Inc. (Nasdaq: TALK) and Brightside Health have announced expansions of services to Medicare and Medicare Advantage.
However, this is enabled by the temporary extension of COVID-era telehealth flexibilities. HHS Secretary Xavier Becerra told a U.S. House of Representatives committee that “we can’t allow those flexibilities to expire” when presenting the Biden administration’s budget for the federal fiscal year 2025.
Further, several U.S. senators have decried so-called ghost or phantom networks — registries of providers that appear to be available to member enrollees but are actually not — and have filed legislation to hold health plans of various types to account for misleading the public.
In March, CMS announced a 2.7% increase in funding for inpatient psychiatric fasciitis for 2025.
Companies featured in this article:
Centers for Medicare & Medicaid Services, Office of Inspector General, U.S. Department of Health and Human Services
